Is Your Hair Loss Normal? Types of Alopecia & When to See a Doctor
Hair is deeply tied to identity. It frames the face, signals youth and vitality, and — for many cultures, including here in the Philippines — carries social and emotional weight that goes far beyond aesthetics. So when clumps appear on the pillow, the shower drain fills faster than usual, or a widening part line stares back from a mirror, the reaction is rarely casual. It's alarming.
Yet hair loss is extraordinarily common. By some estimates, roughly half of all men and a quarter of all women will experience noticeable thinning by middle age. The medical umbrella term for it — alopecia — covers dozens of distinct conditions, from the familiar receding hairline to patchy bald spots to sudden, dramatic shedding. Some forms are temporary and self-correcting. Others are progressive and, without intervention, permanent.
The challenge most people face isn't recognizing that they're losing hair. It's knowing when ordinary shedding crosses the line into something that deserves medical attention — and understanding what a doctor can actually do about it.
How Hair Growth Actually Works
Before you can make sense of hair loss, it helps to understand what "normal" looks like.
Each hair follicle cycles through three phases:
- Anagen (growth phase) — lasts two to seven years. At any given moment, about 85–90% of the hair on your scalp is in this stage.
- Catagen (transition phase) — a brief two-to-three-week period where the follicle shrinks and detaches from the blood supply.
- Telogen (resting phase) — lasts roughly three months. The old hair sits in place until a new anagen hair pushes it out.
Shedding 50 to 100 hairs a day is perfectly normal. That sounds like a lot, but with roughly 100,000 follicles on the average scalp, it's a rounding error. Problems arise when shedding outpaces regrowth, when follicles stop cycling altogether, or when they miniaturize — producing thinner, shorter, weaker hairs with each successive cycle until they essentially give up.
The Most Common Types of Alopecia

Androgenetic Alopecia (Pattern Hair Loss)
This is the big one. It accounts for the vast majority of hair-loss cases in both men and women. In men, it typically presents as a receding hairline and thinning at the crown. In women, the pattern is usually a diffuse thinning across the top of the scalp, with the frontal hairline preserved.
The driver is dihydrotestosterone (DHT), a hormone derived from testosterone. Genetically predisposed follicles respond to DHT by gradually miniaturizing. It's progressive: without treatment, the trend only moves in one direction.
Alopecia Areata
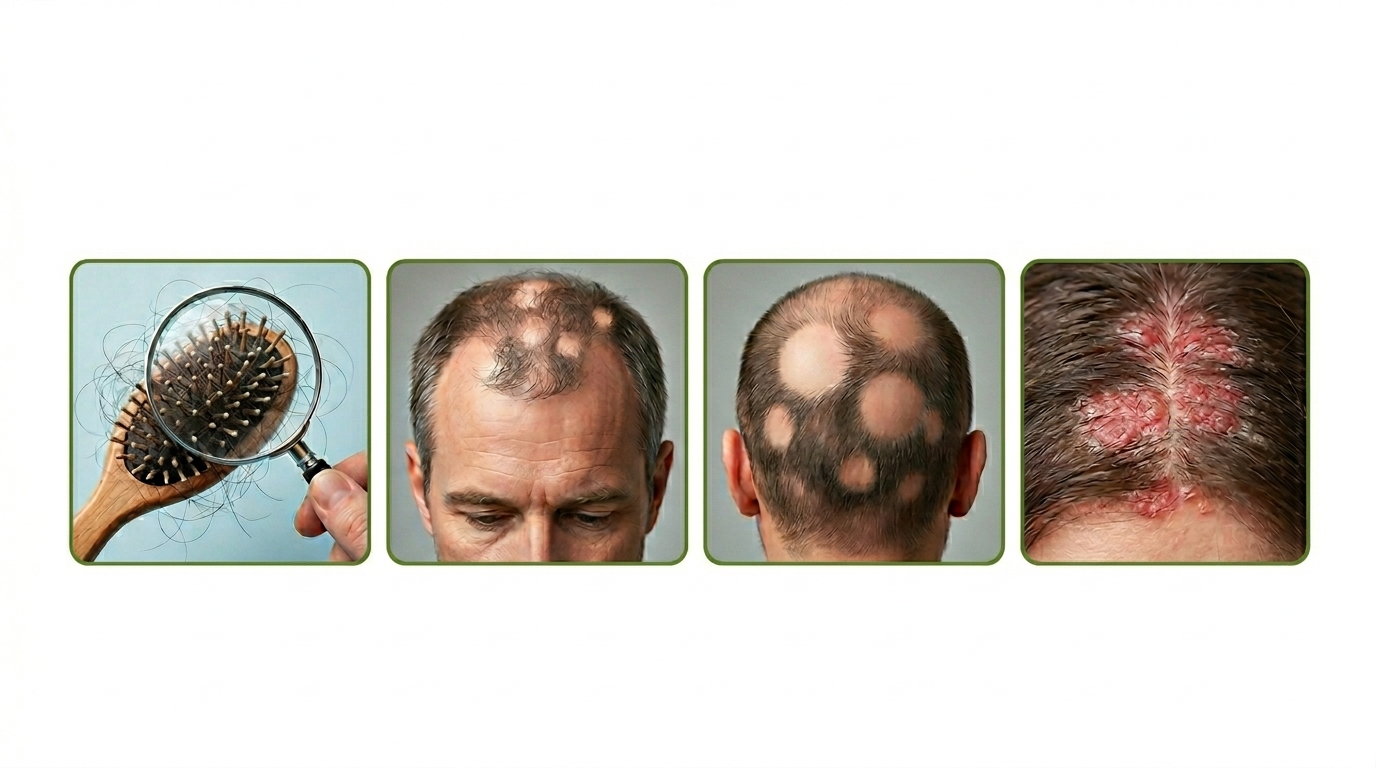
An autoimmune condition in which the body's immune system mistakenly attacks hair follicles, producing smooth, round bald patches — often coin-sized — that can appear suddenly on the scalp, beard, eyebrows, or elsewhere. In more severe forms (alopecia totalis and alopecia universalis), it can lead to total loss of scalp hair or all body hair.
Telogen Effluvium
A reactive form of shedding triggered by a physiological shock — severe illness, major surgery, childbirth, crash dieting, extreme stress, high fever, or certain medications. Large numbers of follicles are prematurely pushed into the telogen phase simultaneously, resulting in dramatic but usually temporary diffuse thinning two to three months after the triggering event.
Traction Alopecia
Caused by sustained tension on the hair — tight ponytails, braids, cornrows, hair extensions, or heavy accessories worn over long periods. It's most common along the hairline and temples and is fully preventable by changing styling habits. Left unchecked, however, the damage can become permanent.
Other Causes
Fungal infections (tinea capitis), scarring conditions like lichen planopilaris, thyroid disorders, iron deficiency, nutritional gaps, and hormonal shifts (such as polycystic ovary syndrome) can all manifest as hair loss. This is precisely why a proper diagnosis matters — the treatment for one condition can be useless or even harmful for another.
When Should You Actually See a Doctor?
Here's the practical heart of the matter. Not every shed hair is a crisis, but certain signals should prompt you to book an appointment with a dermatologist — ideally one experienced in hair and scalp conditions.
1. Sudden or Rapid Shedding
If you notice a dramatic increase in the amount of hair coming out — filling your hands during a shower, covering your clothes, accumulating in visible quantities — within a short window, that pattern points to telogen effluvium or another acute process. While it often resolves on its own, a physician can rule out underlying medical issues like thyroid dysfunction or anemia.
2. Patchy Bald Spots
Smooth, well-defined patches of baldness appearing without warning are the hallmark of alopecia areata. Early treatment can help limit the extent of the loss and speed regrowth.
3. Scalp Changes
Redness, scaling, itching, pain, burning, or pus-filled bumps accompanying hair loss suggest an inflammatory or infectious process — conditions that can scar the follicles permanently if untreated.
4. Progressive Thinning That Concerns You
Even the "slow burn" of androgenetic alopecia benefits from early intervention. The earlier treatment starts, the more hair there is to preserve. Waiting until significant thinning has occurred narrows the options considerably.
5. Hair Loss After Starting a New Medication
Certain drugs — including some blood thinners, antidepressants, beta-blockers, retinoids, and chemotherapy agents — can trigger shedding. Never stop a prescribed medication on your own, but do raise the issue with your prescribing doctor.
6. Hair Loss Accompanied by Other Symptoms
Fatigue, weight changes, irregular periods, joint pain, or skin rashes alongside hair loss can indicate a systemic condition — thyroid disease, lupus, iron deficiency, or a hormonal imbalance — that needs its own treatment.
What to Expect at a Medical Consultation
A dermatologist evaluating hair loss will typically:
- Take a detailed history — onset, pattern, family history, diet, medications, recent illnesses, stress levels, styling habits.
- Perform a clinical examination of the scalp, often using a dermatoscope (a magnifying device with polarized light) to assess follicle density, miniaturization, and scalp skin changes.
- Order blood tests when a systemic cause is suspected — thyroid panel, ferritin, complete blood count, hormonal levels, inflammatory markers.
- In some cases, perform a scalp biopsy — a small tissue sample examined under a microscope — to definitively diagnose scarring alopecias or atypical presentations.
The goal is a specific diagnosis, because treatment varies dramatically by condition.
Treatment Options: A Brief Overview
- Minoxidil (topical) — available over the counter, promotes blood flow to follicles, and is effective for androgenetic alopecia in both sexes. Requires ongoing use; stopping leads to gradual reversal of gains.
- Finasteride / Dutasteride (oral) — prescription DHT blockers used primarily in men with pattern hair loss. Effective but carry a small risk of sexual side effects that should be discussed with your doctor.
- Corticosteroids — injected, topical, or oral, used to suppress the immune response in alopecia areata and some inflammatory conditions.
- JAK inhibitors — a newer class of oral medications (such as baricitinib and ritlecitinib) showing strong results in moderate-to-severe alopecia areata. These have expanded treatment options considerably in recent years.
- Platelet-rich plasma (PRP) therapy — involves injecting concentrated platelets from your own blood into the scalp. Evidence is growing, though protocols vary.
- Hair transplant surgery — relocates DHT-resistant follicles from the back of the scalp to thinning areas. Best suited for stable androgenetic alopecia with adequate donor hair.
- Lifestyle and nutritional support — correcting iron, zinc, vitamin D, or protein deficiencies; managing stress; and eliminating damaging styling practices all play a supporting role.
The Emotional Side Matters Too
It would be incomplete — and honestly, dishonest — to talk about hair loss as a purely clinical matter. The psychological impact is real and well-documented: anxiety, depression, social withdrawal, diminished self-esteem. Studies consistently show that hair loss affects quality of life, and that women and younger patients often bear the heaviest emotional burden.
If hair loss is affecting your mood, your confidence, or how you engage with the world, that alone is a valid reason to seek help. You don't need to wait for a certain percentage of coverage loss or a dramatic before-and-after to "earn" a doctor's appointment. Dermatologists understand the emotional dimension, and many work alongside psychologists or counselors when needed.
The Bottom Line
Hair loss is common, but "common" doesn't mean "ignore it." The single most important thing you can do is get an accurate diagnosis early. Many forms of alopecia respond well to treatment — especially when caught before significant follicle damage occurs. Others, like telogen effluvium, may simply need monitoring and reassurance while the body heals itself.
What doesn't help is guessing, self-treating with unproven supplements or social-media remedies, or waiting years out of embarrassment or the belief that nothing can be done. The science and the treatment landscape have moved meaningfully forward. A conversation with a qualified dermatologist is the first — and most important — step.
Your hair is worth the appointment. And so is your peace of mind.


{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.